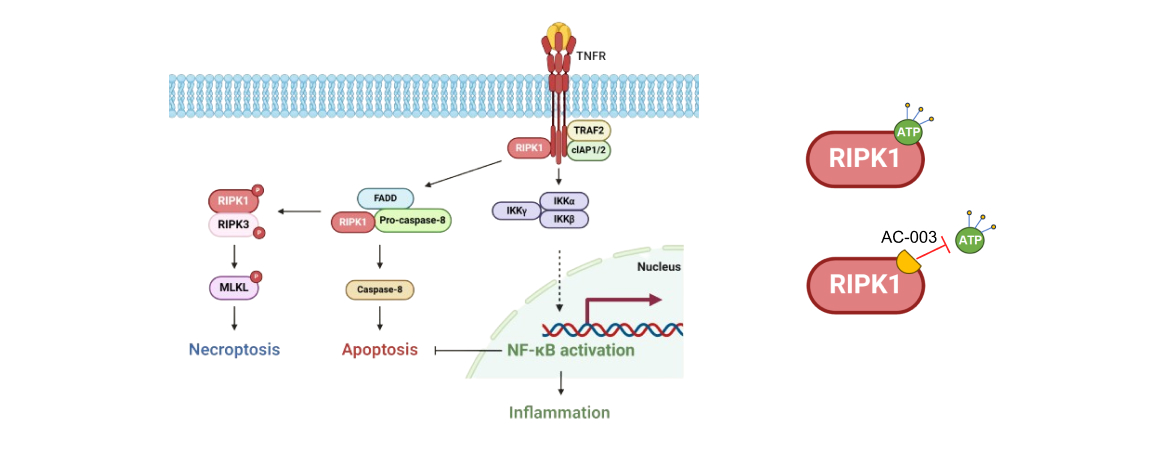
Receptor -interacting protein kinase 1 (RIPK1) is an intracellular adaptor that has been identified in regulating inflammation, apoptosis, and necrosis processes under specific conditions. RIPK1 kinase activity regulates RIPK1-mediated cell death, but is not involved in the regulation of the NF-kB pathway. AC-003, a selective RIPK1 kinase inhibitor, effectively inhibits RIPK1-mediated cell death and inflammation by inhibiting RIPK1 kinase activity. In Phase I study, AC-003 displayed favorable PK characteristics with robust RIPK1 inhibition. AC-003 was safe and well-tolerated with no serious adverse events in healthy subjects. A Phase Ib clinical trial for patients with acute GVHD is currently ongoing.
Graft versus Host Disease (GVHD)
Graft-versus-host disease (GVHD) is a clinical syndrome caused by a reaction of allogeneic donor cells with recipient tissues. It is classified into acute GVHD and chronic GVHD. Acute GVHD is mainly characterized by inflammatory reactions in the skin, gastrointestinal tract, and liver[3]. Chronic GVHD has diverse clinical manifestations involving any one or multiple organs throughout the body[4].
Approximately 38,000 cases of allogeneic hematopoietic stem cell transplantation are performed globally each year. The incidence of acute graft-versus-host disease (aGVHD) requiring systemic treatment is approximately 40~50%[5] , while the incidence of chronic GVHD requiring systematic treatment is around 30-40%[6].
Systemic corticosteroid treatment is the standard of care for GVHD, however, about 50% of GVHD patients will develop steroid-refractory disease[7]. Steroid-refractory GVHD is associated with high mortality, and standard effective treatment has not yet been established. Therefore, the NCCN guidelines recommend that patients participate in well-designed clinical trials to promote further development in disease management and ultimately improve long-term survival for HCT recipients.

Idiopathic Pulmonary Fibrosis (IPF)
Idiopathic pulmonary fibrosis (IPF) is a chronic progressive fibrotic lung disease of unknown etiology.
IPF affects approximately 3 million people worldwide, and the number of patients is increasing. The median survival from diagnosis is only 2 to 3 years. A rapid deterioration in respiratory function within a short period is a significant cause of death in IPF patients[1].
Two anti-fibrotic drugs, Pirfenidone and Nintedanib, have been approved and can delay the loss of function of the lungs, however, overall survival has not been improved.
The hallmark of IPF is irreversible loss of lung function, limited treatment options, and a high mortality rate. The unmet medical needs of IPF patients remain largely unresolved[2].

[1] 中华医学会呼吸病学分会间质性肺病学组,中国医师协会呼吸医师分会间质性肺疾病工作委员会.特发性肺纤维化急性加重诊断和治疗中国专家共识[J]. 2019.
[2] Bramhill C, Langan D, Mulryan H, Eustace-Cook J, Russell AM, Brady AM. Exploration of the unmet needs of patients diagnosed with idiopathic pulmonary fibrosis: a scoping review protocol. BMJ Open. 2023;13(5):e070513.
[3] 黄晓军,吴德沛.中国异基因造血干细胞移植治疗血液系统疾病专家共识(Ⅲ)--急性移植物抗宿主病(2020年版)[J].中华血液学杂志, 2020(7):529-536.
[4] 中华医学会血液学分会造血干细胞应用学组,中国抗癌协会血液病转化委员会.慢性移植物抗宿主病(cGVHD)诊断与治疗中国专家共识(2021年版)[J].中华血液学杂志, 2021, 42(4):11.
[5] Jamy O, Zeiser R, Chen YB. Novel developments in the prophylaxis and treatment of acute GVHD. Blood. 2023;142(12):1037-1046.
[6] Flowers ME, Martin PJ. How we treat chronic graft-versus-host disease. Blood. 2015;125(4):606-615.
[7] NCCN Guidelines Version 1.2024 - Graft-Versus-Host Disease.




